Does Cortisol Affect Testosterone? What Men Over 40 Need to Know About the Cortisol-Testosterone Axis
- Rob Lagana
- Apr 18
- 7 min read

Updated: Apr 19
If you are a man over 40 whose energy, recovery, and training response have all declined at the same time — and you have been told, or suspect, that your testosterone is low — cortisol is almost certainly part of the story. Not as a fashionable stress explanation, but as a direct biological mechanism. The relationship between cortisol and testosterone in men is one of the most well-documented endocrine interactions in the literature, and it is one of the most consistently missed by the commercial men's health industry.
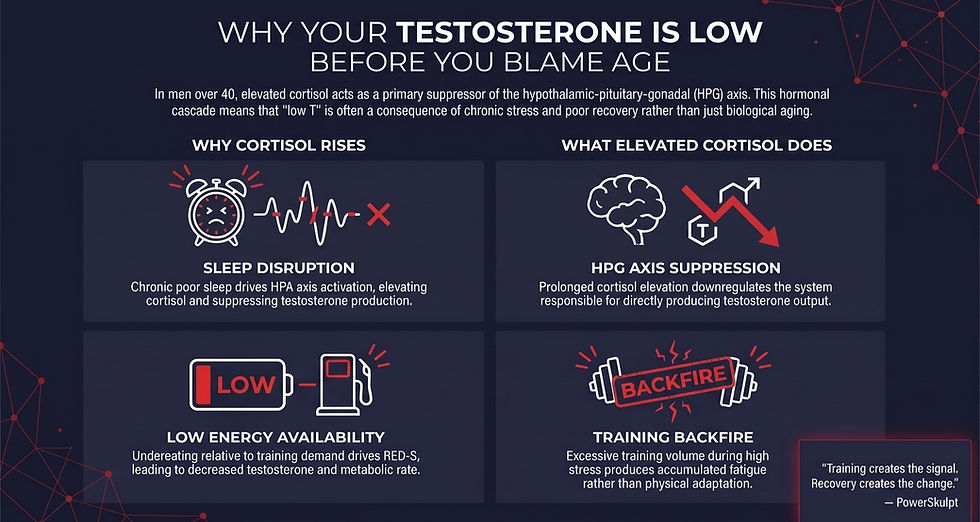
Does cortisol affect testosterone? The short answer is yes — elevated cortisol directly suppresses the hypothalamic-pituitary-gonadal axis, which is the system responsible for producing testosterone. What the research actually shows is more specific than the biohacker framing suggests, and understanding the mechanism is what separates an intelligent response to low energy and stalled progress from a rushed prescription for testosterone replacement that may not address the underlying problem at all.
Does Cortisol Affect Testosterone? The Mechanism in Plain Terms
In a healthy endocrine environment, cortisol and testosterone operate on parallel regulatory systems. Cortisol is produced by the adrenal cortex under direction of the hypothalamic-pituitary-adrenal (HPA) axis. Testosterone is produced primarily by the testes under direction of the hypothalamic-pituitary-gonadal (HPG) axis. Both systems share a common upstream regulator — the hypothalamus — and crosstalk between them is constant.
When cortisol is elevated for prolonged periods, the HPG axis is suppressed. A 2021 primate study published in Frontiers in Physiology demonstrated this directly: adult male rhesus monkeys administered hydrocortisone for 12 days showed significantly increased plasma cortisol and significantly decreased plasma testosterone (Ullah et al., 2021, Frontiers in Physiology). The mechanism has been observed across species and has been documented in human clinical settings through iatrogenic glucocorticoid exposure, where chronic prescribed corticosteroid use produces predictable suppression of testosterone production (Munshi et al., 2018, Case Reports in Endocrinology).
The relevance to men over 40 is this: you do not need to be on prescribed corticosteroids to experience this suppression. Chronic elevation of endogenous cortisol — driven by compressed recovery capacity, sleep disruption, relentless training load, and accumulated life stress — produces the same directional effect, though less dramatically. When cortisol baseline rises and stays elevated over months and years, the HPG axis downregulates.
Testosterone production declines. The man running the system experiences this as fatigue, reduced morning erections, loss of drive, slower recovery, and stalled gains in the gym — and often concludes he needs testosterone replacement when what he actually needs is cortisol regulation.
The Sleep Piece Most Men Ignore
If there is one input that directly determines both cortisol and testosterone for men over 40, it is sleep. And not in the way the sleep-hygiene-blog-post genre tends to describe it.
A 2021 systematic review and meta-analysis in Sleep Medicine examined 18 studies involving 252 men and found that total sleep deprivation — defined as 24 hours or more without sleep — significantly reduced male serum testosterone. Subgroup analysis showed the reduction held at both 24 hours and 40 to 48 hours of total deprivation. Interestingly, short-term partial sleep deprivation did not show a statistically significant effect on testosterone in the same analysis (Su et al., 2021, Sleep Medicine).
The honest reading of this evidence is that occasional late nights are not testosterone-killers. What the broader literature shows, however, is that chronic poor sleep quality — the kind most over-40 men experience over years — drives cortisol elevation through HPA axis activation, which in turn suppresses testosterone through the mechanism described above. A 2020 review in the Journal of Circadian Rhythms traces this cascade explicitly:
sleep disturbance activates the HPA axis, increases corticosteroid production, and suppresses testosterone output (Lateef & Akintubosun, 2020, Journal of Circadian Rhythms).
Middle-aged and older men sleep worse than they did in their twenties — less deep sleep, more awakenings, earlier wake times — and this degradation of sleep architecture is one of the most direct contributors to the cortisol-testosterone imbalance most men are experiencing without naming it. Fixing sleep is not a wellness recommendation. It is a testosterone protocol.
Why "Training Harder" Often Makes Low Testosterone Worse
Here is where men with a training background get into the most trouble. When energy and drive decline, the instinct — backed by decades of fitness culture — is to train harder, eat less, and push through. For a man in his late thirties and older with elevated baseline cortisol, this protocol can accelerate the very suppression it is trying to solve.
The evidence for this comes from endurance sport research, where low energy availability (LEA) — the condition of insufficient energy intake relative to training demand — has been shown to correlate with decreased testosterone levels, decreased bone density, and decreased resting metabolic rate in endurance-trained men (Cupka & Sedliak, 2023,
European Journal of Translational Myology). This is known in sports medicine as Relative Energy Deficiency in Sport (RED-S). The population most affected is not elite athletes. It is high-volume recreational and enthusiast trainers who are chronically underfueled relative to their training load — a profile many over-40 men fit perfectly without recognizing it.
The practical implication: if you are training five or six days a week, restricting calories to stay lean, sleeping poorly, managing career and family stress, and wondering why your drive has collapsed — the answer may not be a testosterone prescription. The answer may be a reduction in training load, an increase in caloric availability, and a serious investment in sleep. This is the same logic that underlies why training harder stops working after 40, expressed through the specific mechanism of HPG axis suppression.
The Commercial "Low T" Problem Men Over 40 Should Know About
The men's health industry has an honesty problem, and it is one the peer-reviewed literature is now openly addressing. A 2024 article in the Journal of the Endocrine Society explicitly named "pseudo-endocrine disorders" — conditions promoted online and in commercial clinics that lack rigorous clinical validation. Among the specific examples discussed: commercial "men's health" clinics that diagnose "low T" without proper hormone testing and prescribe supraphysiologic testosterone therapy that suppresses endogenous testosterone production, leads to a lifelong need for therapy, and carries multiple downstream risks (McDermott, 2024, Journal of the Endocrine Society).
This is not an argument against testosterone replacement therapy when it is genuinely indicated. For men with clinically confirmed hypogonadism — established through multiple morning testosterone draws, LH and FSH measurement, and proper endocrinological evaluation — TRT can be life-changing when prescribed and monitored by a qualified physician. What the paper argues against is the casual commercial diagnosis model, where symptoms alone trigger a prescription without the underlying cause being established. A man with stress-driven, sleep-driven, training-driven cortisol elevation who is given exogenous testosterone may feel better in the short term while his own testicular function quietly shuts down and his underlying cortisol problem persists unaddressed.
The defensible position for a high-performing man over 40 is this: if your testosterone appears low, the first questions are about cortisol, sleep, training load, and life stress — not about TRT dosing. Establish the endocrine environment first. Work with a qualified physician for proper diagnostics. Understand that the commercial men's health space has economic incentives that do not always align with your long-term health.
What Actually Supports Healthy Testosterone in Men Over 40
Based on the research, four inputs consistently support the cortisol-testosterone axis:
Protect sleep as an endocrine protocol, not a lifestyle preference. The evidence linking sleep to both cortisol regulation and testosterone production is among the strongest in the literature. Prioritize sleep duration, sleep timing, and sleep environment. For men with significant sleep disturbance, a sleep study should precede a testosterone prescription.
Calibrate training volume to current recovery capacity. This does not mean stop training. It means stop training as if the 30-year-old body is still running the system. Fewer, better sessions with genuine recovery between them. This is the foundation of smart training after 40.
Address chronic under-fueling. Many men over 40 are chronically restricting calories to stay lean and inadvertently driving LEA and its downstream hormonal consequences. Adequate energy availability is not a bodybuilding concept. It is a testosterone concept.
Pursue proper clinical diagnostics before accepting a TRT prescription. Multiple morning testosterone measurements. LH and FSH. Full thyroid panel. Sleep assessment. A qualified endocrinologist or men's health specialist — not a commercial clinic — as the diagnostic partner.
What the research does not support: "natural testosterone boosters," ashwagandha protocols marketed as T-boosters, and the entire "lower your cortisol with this supplement stack" genre. None of these address the underlying cortisol-testosterone axis in a way the evidence validates. Most of them are marketing solutions to problems they cannot actually solve.
The PowerSkulpt Framework
The PowerSkulpt approach to the cortisol-testosterone axis in men over 40 is built around a single premise: the hormonal environment is upstream of everything. Before considering replacement therapy, restore the environment that should be producing testosterone in the first place. In practice, this means calibrated training volume, clinical-grade sleep protection, adequate nutrition, and nervous system regulation. When these are in place, a significant percentage of men who were convinced they needed TRT find their own endocrine system returning to function.
This is the framework the Protocol Briefing lays out in detail. It is not a testosterone-boosting protocol. It is the architecture that allows the over-40 male body to operate in a more regulated state, which supports testosterone as a consequence.
For men who see the same pattern on the muscle-building side, how to build muscle after 40 traces the same biology from a different angle.
Training creates the signal. Recovery creates the change.
Most programs start with training. PowerSkulpt starts with recovery.
The Next Step
If you are an over-40 man navigating stalled energy, reduced drive, and the question of whether you need TRT, the Protocol Briefing is the fastest way to see what a recovery-first framework looks like in practice. Five minutes. Free. It outlines the endocrine architecture most programs ignore.
If you want a direct, one-to-one review of where your current approach may be undermining your own testosterone production, the PowerSkulpt Advanced Consultation is a 60-minute private session — $300 CAD, includes a 7-day follow-up — where we map your specific situation and define next steps. Email to inquire.
References
All claims in this post are based on articles retrieved from PubMed.
Ullah R, Naz R, Batool A, et al. RF9 Rescues Cortisol-Induced Repression of Testosterone Levels in Adult Male Macaques. Frontiers in Physiology. 2021;12:630796. https://doi.org/10.3389/fphys.2021.630796
Munshi LB, Tsushima Y, Cheng K, Brito M. Megestrol Acetate-Induced Symptomatic Hypogonadism in a Male Patient. Case Reports in Endocrinology. 2018;2018:7048610. https://doi.org/10.1155/2018/7048610
Su L, Zhang SZ, Zhu J, Wu J, Jiao YZ. Effect of partial and total sleep deprivation on serum testosterone in healthy males: a systematic review and meta-analysis. Sleep Medicine. 2021;88:267-273. https://doi.org/10.1016/j.sleep.2021.10.031
Lateef OM, Akintubosun MO. Sleep and Reproductive Health. Journal of Circadian Rhythms. 2020;18:1. https://doi.org/10.5334/jcr.190
Cupka M, Sedliak M. Hungry runners - low energy availability in male endurance athletes and its impact on performance and testosterone: mini-review. European Journal of Translational Myology. 2023;33(2). https://doi.org/10.4081/ejtm.2023.11104
McDermott MT. Pseudo-endocrine Disorders: Recognition, Management, and Action. Journal of the Endocrine Society. 2024;9(1):bvae226. https://doi.org/10.1210/jendso/bvae226