How to Reduce Cortisol in Menopause: The Biological Reasons Your Workouts Now Backfire
- Rob Lagana
- Apr 18
- 7 min read

Updated: Apr 19
If you are a woman in perimenopause or menopause who has watched your workouts stop producing results — or started producing the opposite of what they used to — cortisol is almost certainly part of the story. Not because you are stressed in the way the wellness industry means it. Because the hormone that once helped you adapt to training has shifted its baseline, and the system that once regulated it has lost one of its key buffers.
How to reduce cortisol in menopause is not a question of meditation apps, adaptogen supplements, or "learning to relax." It is a question of understanding what specifically changed in your endocrine system, why the same training no longer produces the same result, and which inputs the research actually supports for bringing the system back into regulation.
How to Reduce Cortisol in Menopause Starts With Understanding What Changed
Cortisol is a regulatory hormone. In a healthy system, it rises sharply in the morning — the cortisol awakening response — falls across the day, and bottoms out at night to allow deep sleep. The rhythm matters as much as the absolute level.
What the research shows is that this rhythm changes measurably across perimenopause. In the Swiss Perimenopause Study, researchers followed 127 women aged 40 to 56 for 13 months, assessing salivary cortisol, estradiol, and progesterone at multiple timepoints. They found that cortisol levels increased over the course of the study, while estradiol and progesterone showed the highly variable decline pattern typical of the menopause transition (Grub et al., 2021, Frontiers in Global Women's Health).
This is the finding that most over-40 women have never been told: during perimenopause, cortisol is not responding to a stressful life. It is rising as a function of the hormonal transition itself.
Two mechanisms appear to drive this:
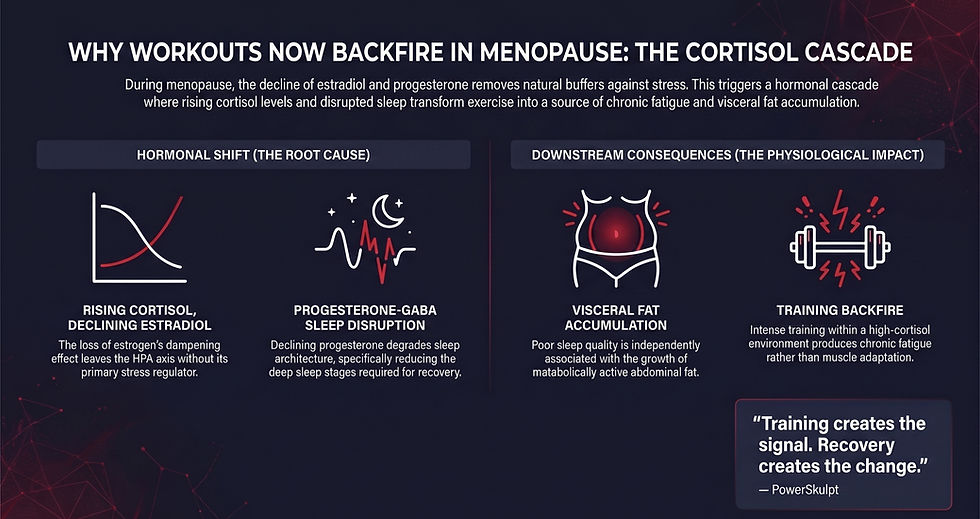
Estrogen withdrawal removes a dampening input to the HPA axis. Estrogen has a moderating effect on hypothalamic-pituitary-adrenal axis activity, the system that regulates cortisol release. As estradiol declines, the HPA axis loses one of its stabilizing signals.
Vasomotor symptoms correlate with HPA axis alteration. In a study of 101 perimenopausal women aged 45 to 55, those with more frequent and severe hot flashes showed a blunted cortisol awakening response — a marker of HPA axis dysregulation — independent of sleep quality, estrogen, and progesterone levels (Sauer et al., 2020, Menopause). Hot flashes and cortisol dysregulation appear to track together.
The practical implication: in menopause, elevated cortisol is not a personal failing. It is a predictable physiological signature of a transition your endocrine system is navigating.
The Sleep-Cortisol Loop Conventional Programs Ignore
One of the most consequential changes in perimenopause is what happens to sleep — and what poor sleep does to the rest of the system.
Progesterone has a quieting effect on the central nervous system through its metabolites' positive allosteric modulation of the GABA-A receptor. A 2021 systematic review and meta-analysis in the Journal of Clinical Endocrinology and Metabolism examined randomized controlled trials of micronized progesterone supplementation in postmenopausal women and found it improved several sleep parameters, including sleep onset latency (Nolan et al., 2021, JCEM). The conclusion points to what women lose as progesterone declines: a natural GABA-supporting signal that helps the nervous system downregulate at night.
This matters beyond subjective sleep quality. A study in Psychoneuroendocrinology examining 101 adults found that poor sleep quality was associated with significantly greater visceral fat — but not greater total body fat (Sweatt et al., 2018, Psychoneuroendocrinology). The body composition penalty from disrupted sleep shows up specifically in the metabolically active abdominal depot. For perimenopausal women already experiencing estrogen-driven fat redistribution toward the abdomen, the sleep disruption compounds the problem.
So the loop closes on itself: progesterone declines, sleep quality deteriorates, visceral fat accumulates, cortisol stays elevated, nervous system regulation further deteriorates. Each piece reinforces the others. This is what most over-40 women are experiencing — not a willpower problem but a compounding biological cascade.
Why Training Harder Backfires — and Why Training Smarter Works
Here is where the conventional advice collides with the biology. When fat loss stalls, most women are told to train more intensely, eat less, or both. In a menopausal endocrine environment, this is often the wrong lever to pull.
The reasoning is not that acute exercise causes catastrophic cortisol spikes. In fact, a 2024 study in Endocrine Research found that a six-month intervention combining weight loss and aerobic exercise training in postmenopausal women with overweight and obesity produced significant weight loss but did not significantly change basal cortisol concentrations (Ryan et al., 2024, Endocrine Research). Exercise is not the enemy. The issue is the context in which that exercise lands.
The menopausal body begins with an elevated baseline cortisol environment, disrupted sleep, and compromised recovery capacity. When chronic high-intensity training is added to that environment without calibration, the result is not adaptation — it is accumulated fatigue that further dysregulates the system. This is why many women feel worse, not better, when they respond to stalled progress by adding more training volume.
What the research on exercise intervention in postmenopausal women consistently supports is that structured, moderate-intensity training produces meaningful metabolic and cardiovascular improvements — without the cortisol-spiking consequences of chronic overreach. Elevated cortisol itself is clinically associated with increased visceral fat and decreased skeletal muscle mass, even at subtle levels of cortisol elevation (Delivanis et al., 2021, European Journal of Endocrinology). Training that respects this biology rather than fighting it is what produces results in menopause.
This is the same recovery-first logic that explains why training harder stops working after 40, and why recovery — not calories — drives fat loss in midlife. The cortisol context is the reason.
What the Evidence Actually Supports for Reducing Cortisol in Menopause
Based on the research, four inputs consistently support cortisol regulation during the menopause transition:
Protect sleep as a clinical priority, not a lifestyle preference. Given the progesterone-GABA pathway, sleep is where menopause most directly undermines nervous system regulation. Consistent sleep timing, a cool dark sleep environment, and limiting late-evening stimulants are not soft advice — they are addressing the biology.
Calibrate training volume to current recovery capacity. This is not a call to stop training. It is a call to stop training as if the 35-year-old body is still the one running the program. For most women in perimenopause and menopause, fewer well-structured sessions with genuine recovery between them outperform high-frequency moderate-effort training.
Address visceral adiposity through resistance training and nutrient timing, not through aggressive calorie restriction. Aggressive restriction drives cortisol in the wrong direction. Resistance training supports muscle retention, which supports insulin sensitivity, which reduces the hormonal environment that drives visceral fat storage.
Discuss progesterone and hormone therapy with a qualified clinician. The Nolan meta-analysis is strong evidence that micronized progesterone supports sleep in postmenopausal women. This is not a recommendation to self-prescribe — it is a recommendation to have an informed conversation with a menopause-literate physician, which remains one of the highest-leverage steps most women over 40 have never taken.
What the research does not support: generic "lower your cortisol" protocols built on supplements, meditation apps, or adaptogen stacks promoted by wellness influencers. None of these address the underlying hormonal transition. Most of them are addressing a problem the woman does not actually have.
The PowerSkulpt Framework
The PowerSkulpt approach to cortisol regulation in menopause is built around a single premise: the hormonal environment is non-negotiable, but the inputs into that environment are. When recovery capacity is restored — through calibrated training volume, clinical-grade sleep protection, appropriate nutritional support, and nervous system work — the body begins responding the way it did before the transition started exerting its pressure.
This is the framework the Protocol Briefing lays out in detail. It is not a cortisol-lowering protocol. It is the architecture that allows the menopausal body to operate in a more regulated state, which reduces cortisol as a consequence rather than as a target.
For women who see this pattern mirror in weight loss frustration specifically, the biological reasons conventional programs fail for women over 40 traces the same territory from a different direction.
Training creates the signal. Recovery creates the change.
Most programs start with training. PowerSkulpt starts with recovery.
The Next Step
If you are navigating the cortisol side of menopause and the conventional advice has stopped producing results, the Protocol Briefing is the fastest way to see what a recovery-first framework looks like in practice. Five minutes. Free. It outlines the architecture most programs ignore.
If you want a direct, one-to-one review of where your current approach is breaking down, the PowerSkulpt Advanced Consultation is a 60-minute private session — $300 CAD, includes a 7-day follow-up — where we map your specific situation and define next steps. Email to inquire.
References
All claims in this post are based on articles retrieved from PubMed. Direct links provided:
Grub J, Süss H, Willi J, Ehlert U. Steroid Hormone Secretion Over the Course of the Perimenopause: Findings From the Swiss Perimenopause Study. Frontiers in Global Women's Health. 2021;2:774308. https://doi.org/10.3389/fgwh.2021.774308
Sauer T, Tottenham LS, Ethier A, Gordon JL. Perimenopausal vasomotor symptoms and the cortisol awakening response. Menopause. 2020;27(11):1322-1327. https://doi.org/10.1097/GME.0000000000001588
Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data. The Journal of Clinical Endocrinology and Metabolism. 2021;106(4):942-951. https://doi.org/10.1210/clinem/dgaa873
Sweatt SK, Gower BA, Chieh AY, Liu Y, Li L. Sleep quality is differentially related to adiposity in adults. Psychoneuroendocrinology. 2018;98:46-51. https://doi.org/10.1016/j.psyneuen.2018.07.024
Ryan AS, Serra MC, Bigman G, Jaber S. The Effects of Weight Loss and Aerobic Exercise on Cortisol and Cortisol Suppression in Postmenopausal Women with Overweight and Obesity. Endocrine Research. 2024;50(2):87-95. https://doi.org/10.1080/07435800.2024.2439408
Delivanis DA, Hurtado Andrade MD, Cortes T, et al. Abnormal body composition in patients with adrenal adenomas. European Journal of Endocrinology. 2021;185(5):653-662. https://doi.org/10.1530/EJE-21-0458