Cortisol and Menopause: The Hormonal Connection Most Programs Miss
- Rob Lagana
- May 8
- 6 min read

The most misdiagnosed hormonal pattern in midlife women is not estrogen decline. It is the cortisol shift that happens alongside it.
Most women in perimenopause or menopause who walk into a fitness program with weight gain, sleep disruption, and stalled training results are told the problem is hormonal. That is correct. They are told the relevant hormone is estrogen. That is incomplete. The hormonal connection driving most of what they are experiencing — the visceral fat, the wired-but-tired evenings, the workouts that no longer produce results — is the relationship between cortisol and menopause that conventional programs almost universally miss.
This post explains what that connection actually is, why it matters more than most realize, and why training harder against it makes the situation worse.
For the broader explanation of why cortisol regulation shifts in midlife in the first place, see Cortisol and Menopause: The Hormonal Connection Most Programs Miss

How Cortisol and Menopause Are Biologically Linked
Cortisol does not operate in isolation. It exists within a regulatory system shaped by other hormones — and estrogen is one of the most important regulators of cortisol behavior in the female body.
Across the reproductive years, estrogen exerts a buffering effect on the hypothalamic-pituitary-adrenal axis — the system that produces and regulates cortisol. Estrogen modulates how the brain perceives stress, how the adrenal glands respond, and how quickly elevated cortisol returns to baseline after a stressor. It also influences the binding proteins that determine how much cortisol is biologically active at any given moment.
When estrogen declines through perimenopause and into menopause, this regulatory architecture changes. Cortisol baseline tends to rise. The cortisol awakening response — the natural surge that occurs in the first 30-45 minutes after waking — becomes elevated and prolonged. Stress recovery slows. The same psychological or physical stressor that produced a clean cortisol spike-and-recovery curve at 38 produces a higher peak and a longer tail at 48.
This is not a malfunction. It is the predictable consequence of removing one of the system's most important moderators.
The clinical literature has documented this pattern consistently. Postmenopausal women show elevated 24-hour cortisol output compared to premenopausal women, even when controlling for stress exposure, sleep quality, and body composition. The cortisol-estrogen relationship is not theoretical. It is measured.
Why Cortisol Menopause Patterns Get Misdiagnosed
The reason this connection is missed in most fitness and wellness programs is structural, not informational.
Most fitness programs treat cortisol as a stress problem rather than a hormonal one. The recommendations focus on stress management techniques — meditation, breathwork, journaling — without addressing the underlying biology of why cortisol regulation has changed in the first place. These techniques have value. They are also insufficient when the issue is not psychological stress but a regulatory shift in how the body produces and clears cortisol.
Most menopause programs treat estrogen as the dominant hormonal variable. They focus on hot flashes, mood, libido, and bone density. These are real and important. They are also incomplete pictures of what is happening hormonally. The cortisol shift is happening simultaneously and is often the more immediate driver of the symptoms women describe as "menopause weight gain" — particularly visceral adiposity around the midsection, which is a cortisol pattern more than an estrogen pattern.
Most physicians, unless specifically trained in functional or integrative endocrinology, do not test cortisol in midlife women presenting with weight gain or training plateaus. The standard panel runs estrogen, progesterone, FSH, and thyroid. Cortisol testing — particularly the diurnal cortisol pattern that would actually reveal dysregulation — is rarely ordered. The data that would identify the issue is not collected, so the issue is not identified.
The result is a generation of high-performing women in midlife being given partially correct advice. Yes, your hormones are changing. No, the relevant hormone is not only the one your wellness app talks about.
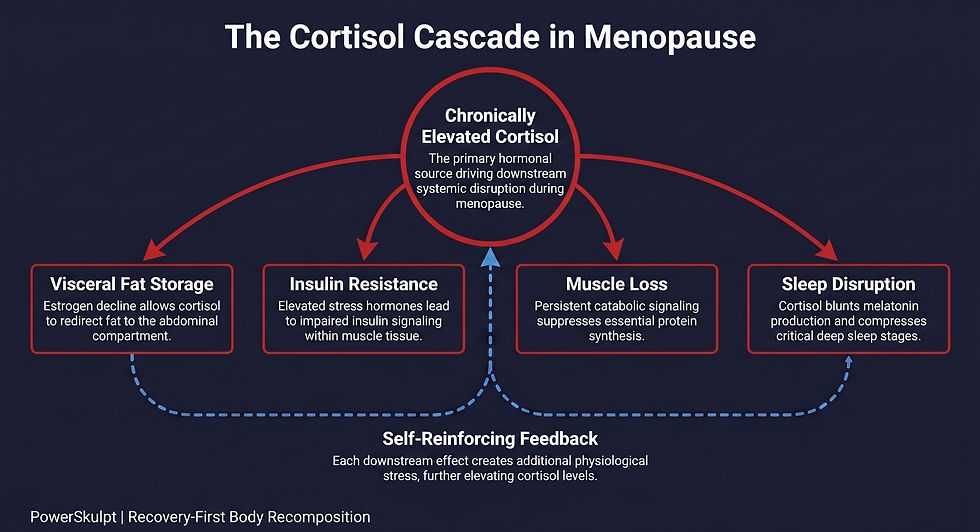
The Cortisol Cascade That Drives Menopause Weight Gain
Once cortisol baseline shifts upward in perimenopause and menopause, a predictable cascade follows. This is the cascade that produces what most women describe as menopause weight gain — but the mechanism is cortisol, not estrogen alone.
Visceral fat storage increases. Cortisol drives fat storage preferentially to the abdominal region, particularly the deep visceral compartment. This is why so many women in midlife describe weight gain that "settles in the middle" despite no significant change in eating patterns. The fat is not simply being added; it is being relocated by hormonal signaling.
Insulin sensitivity decreases. Chronically elevated cortisol impairs insulin signaling, particularly in muscle tissue. This means the same carbohydrate intake produces a higher glucose excursion and a longer insulin response. Over time, this reduces metabolic flexibility and makes fat oxidation harder.
Muscle protein synthesis is suppressed. Cortisol is a catabolic hormone. When elevated chronically, it reduces the body's capacity to build and maintain lean tissue — the same lean tissue that becomes harder to preserve in midlife due to declining anabolic signaling. This is why so many women report "doing the same workouts but losing muscle." The training input has not changed. The hormonal environment that translates that input into adaptation has.
Sleep architecture deteriorates. Cortisol and melatonin operate in a reciprocal rhythm. When cortisol is elevated in the evening — a common pattern in midlife women — melatonin release is blunted, sleep onset is delayed, and the deep-sleep phases that drive recovery are compressed. This is the biology behind the wired-but-tired pattern most perimenopausal women recognize immediately.
Each of these effects compounds. Visceral fat itself is metabolically active and contributes to further cortisol dysregulation. Poor sleep elevates next-day cortisol. Reduced muscle mass lowers metabolic rate. The system reinforces itself.
This is why "eat less and exercise more" produces such poor results in this population. The advice does not address the cascade. It often accelerates it.
Why Training Harder Against Cortisol Menopause Makes It Worse
The instinct, when results stall, is to train harder. Add another session. Push the cardio. Cut the calories.
In a younger woman with intact estrogen-cortisol regulation, this can work. The system absorbs the additional stress, recovers, and produces adaptation. In a woman with shifted cortisol baseline due to menopause, this same approach lands very differently. Each additional training session adds to a cortisol load the system is no longer clearing efficiently. Recovery is incomplete. Sleep does not fully restore. Cortisol baseline rises further. Visceral fat storage accelerates rather than reverses.
This is the clinical pattern PowerSkulpt sees most consistently in midlife women: discipline producing the opposite of the intended result. The training input is correct by the standards of every program they have ever followed. The biology has changed underneath the input.
This is also why why is it harder to lose weight after 40 for women is one of the most-searched questions in this demographic. The answer is rarely a willpower issue. It is almost always a recovery and hormonal regulation issue.
The PowerSkulpt approach treats cortisol regulation as a precondition for fat loss rather than a consequence of it. Training is reduced, not increased. Sleep is prioritized as a primary intervention, not a secondary one. Nutrition is structured to support cortisol clearance rather than create additional metabolic stress. This is the framework explored across the recovery-first model that actually works and the body recomposition timeline after 40.
What this looks like in practice — the testing, the protocol structure, the specific interventions that address cortisol-menopause patterns — is detailed in the companion post: how to reduce cortisol in menopause.
The two posts work together. This one explains what is happening. That one explains what to do about it.
For the female-specific timeline broken out by hormonal stage, see how long does body recomposition take for women over 40.
What This Means for High-Performing Women in Midlife
If you are a high-performing woman in perimenopause or menopause whose results have stalled despite doing everything correctly, the most useful diagnostic question is not "am I working hard enough?" It is "what is my cortisol doing?"
The signs of cortisol-menopause dysregulation are usually identifiable without expensive testing, though testing helps. They include visceral weight gain that does not respond to caloric restriction, sleep that is shorter and less restorative than it used to be, training sessions that produce more fatigue than adaptation, and a persistent wired-but-tired quality in the late afternoon and evening. If three or more of these are present, cortisol is almost certainly contributing — and addressing it should be upstream of any further training intensification.
This is why the PowerSkulpt approach starts with recovery rather than training, with cortisol regulation rather than caloric restriction, and with biological assessment rather than program intensification. The biology has changed. The methodology must change with it.
Training creates the signal. Recovery creates the change.
Most programs start with training. PowerSkulpt starts with recovery.
For a direct clinical assessment of cortisol-menopause patterns and what your specific biology requires, the PowerSkulpt Advanced Consultation is a 60-minute private session focused on your current hormonal environment, recovery capacity, and protocol design. Investment: $300.